Discrimination double chamber, atrial tachycardia, Onset/Stability
Tracing
Manufacturer Boston Scientific
Device ICD
Field Discrimination
N° 6
Patient
This 76-year-old man underwent implantation of a Cognis triple chamber defibrillator for primary prevention, in the context of ischemic cardiomyopathy with wide QRS complex. He was seen for a routine follow-up visit.
Summary
Episode diagnosed in the VT zone with atrial rate = ventricular rate; the programmed discriminator was Onset/Stability.

Graph and trace
Tracing
- rapid ventricular rhythm with 1:1 A:V ratio, at the limit of the VT zone (marker RVS);
- slight acceleration of the rate into the VT zone (limit of the VT zone = 375 ms);
- 8 out of 10 criterion fulfilled. The analysis of the arrhythmia onset was in favor of sinus tachycardia (Gradl: gradual onset);
- at the end of Duration, the rhythm was considered stable (probable sinus tachycardia). Consequently, no therapy was delivered;
- continuation of the analysis of stability cycle by cycle; the rhythm remained stable and the therapies were inhibited.
Other articles that may be of interest to you


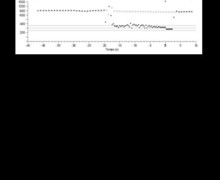

This episode was diagnosed as sinus tachycardia because the rhythm was stable with a gradual onset; therefore, the therapies were inhibited. It was, in fact, an episode of sustained atrial tachycardia with 1:1 AV conduction. The rate of the tachycardia hoovers around the lower limit of the VT zone, explaining the gradual interpretation of the onset. The ventricular rate varied very slightly, though oscillated between the sinus and the VT zones. This patient’s rhythm evolved in a first stage from 60 bpm (resting rate) to 165 bpm. The rate of the tachycardia gradually accelerated further to reach the VT zone. The sudden onset was not diagnozed by the device. Fortuitously, the unrecognized sudden onset spared the patient the delivery of inappropriate therapies. The 1:1 atrial tachycardia was, indeed, accurately discriminated neither by the V>A relationship (in a 1:1 atrial tachycardia, as in VT with 1:1 retrograde conduction, the atrial rate the same as the ventricular rate), nor by sudden onset (the onset of an atrial tachycardia, like that of VT, is most often gradual) nor by stability (as with VT, the ventricular rate of an atrial tachycardia is most often stable).
In this patient, a) the VT zone could be raised to avoid an overlap between the diagnostic zone and the zones of the clinical atrial tachycardia, or b) a discrimination based on Rhythm ID could be given priority.